If there’s one thing that’s treated as certain in debates over California’s mental health system, it’s that the state doesn’t have enough psychiatric beds.
The state de-institutionalized people living in (or, perhaps, abandoned into) state hospitals more rapidly—and from a lower baseline—than the national average:

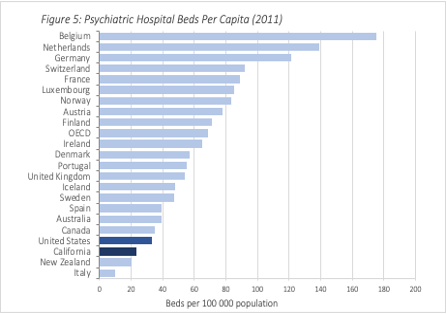
Today, California has fewer psychiatric beds per capita than the national average. According to a widely-cited report from the National Association of State Mental Health Directors, the figure 23 per 100,000, versus a national average of 33. SAMSHA in 2018 reports a similar number: 27.7, which has been picked up by some critics of California’s mental health system. The medical director of California’s state hospital system puts the figure at only 17. This puts it way below virtually every European country, as reported by the OECD.
The closest I’ve achieved to mental health policy celebrity was when the following chart, from my report on California’s conservatorship system, was presented in a San Francisco Board of Supervisor’s meeting, which shows this pretty starkly:
* * *
The problem is that I’m pretty sure my figure and the claims of all the authors above is wrong. Weirdly, the NASMHD report which most people (including myself!) cite has a very different number for the residents of psychiatric hospitals at a given point in time (34.5) than the number of beds (23.5). Nationally, these two numbers are almost the exact same in their data (31.6 and 33.1, respectively). So of the disparate California numbers, which one is more accurate?
If you do some manual calculations, it’s clearly the larger one. The California Hospital Association counts 6,777 acute non-state psychiatric beds in 2019 (CHA’s acute bed list is more-or-less consistent with the number of beds licensed by DHCS to take involuntary patients, although smaller because not all psych hospitals do). The State Hospitals report a daily census of 6,122 in 2020, which is not that far from other sources, like the Treatment Advocacy Center, which reported 5,905 in 2016 (the number of state beds in California has been going up). If you add those two up, and divide them by the California population in 2019, you end up with 32.6 per 100,000—the higher number.
It also turns out that other OECD counties have been downsizing their inpatient capacity since 2011. A more accurate chart winds up looking like this:

California winds up quite close to countries that Bernie Sanders tells us have great health systems, like the UK or Canada, and is not far from the Scandinavian countries that have great social service systems, like Iceland or Sweden. California also has a network of Mental Health Rehabilitation Centers (IMDs) that don’t go into that number because they’re not acute hospitals. But they are locked places where people are required to take medication, and thus are kind of close. With them, California has 36/100,000—about the same number of inpatient beds as the UK.
* * *
Why does this matter? These numbers get thrown as an explanation for where California went wrong, but those arguments need to be revisited if California is not, in fact, an outlier. It’s harder to argue that the current state of California’s streets is because of a lack of psychiatric beds if the state doesn’t have particularly few of them. My own sense is that it’d be better to focus on the rise of meth and fentanyl, the state’s housing crisis and highest-in-the-nation real poverty rate, and the consequences of creating a mass incarceration monster and then (thankfully) decarcerating, albeit without creating supports in the community. Although groups like TAC claim that 50 beds per 100,000is the necessary minimum, the evidence for this is not extensive. There are many robust mental health systems with about the same number of beds as California, and some (like Trieste, in Italy) with virtually none.
Our fixation on the quantity of beds often overlooks issues of who controls those beds, how are they used, and what is the quality of care attached to them. California may not have particularly few beds, but the ones it has are disproportionately controlled by private and for-profit providers:
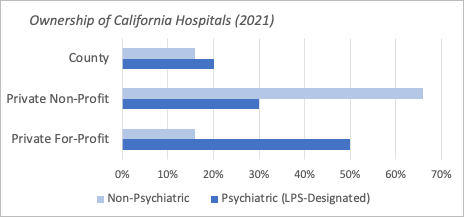
There’s consistent evidence that closing public psychiatric beds is correlated with increases in homelessness and incarceration, although by all accounts this explains only a small portion of both. My own research on conservatorship has found that private hospitals, particularly for-profit ones, are reluctant to provide costly, long-term care to people with the most chronic illnesses (whether they provide better is open for debate). Meanwhile, California may have a comparatively large number of public, state hospital beds, but a huge proportion of them are going towards forensic patients (more so than in other states).
It might also be the case that California’s psychiatric beds are used particularly ineffectively. There’s no good national data on lengths of stay, but research has shown that slightly longer hospitalizations reduce readmissions (they also may increase deaths by suicide post-hospitalization). California’s involuntary commitment laws are not particularly strict on the front end, but make keeping people rapidly more and more administratively complex and costly. It might be that the state is cycling people in and out on involuntary holds at a faster rate (which is how you wind up with hundreds of people in LA who have been involuntarily held 50+ times). It also has made voluntary hospitalization essentially a non-option for the Medi-Cal population, i.e. the people most vulnerable to mental illness.
That said, even if a lack of beds didn’t cause what is widely (and in my view, accurately) described as a crisis, building more may be necessary to get out of it. This summer, I followed outreach teams in LA working with “super” high utilizers of jails, hospitals, and ERs. I could imagine a time in the past where these individuals would have accepted an offer of permanent supported housing and intensive outpatient supports, which is usually presented as the gold standard of care for people living with severe and persistent mental illness. But we didn’t offer it, and now they’ve been burned and abandoned by the system for so long that there’s nothing they’ll accept from it.
Still, as lawmakers and advocates go into a legislative session where “building beds” is one option on the table, it’d be useful to start from an accurate baseline and a recognition that a “bed” can mean anything from a mattress in a crummy locked sub-acute facility to a spot in high quality “Housing that Heals.” We should be asking which beds and not just how many.

8 thoughts on “How many psychiatric beds does(n’t) California have?”